

Understanding Shoulder Pain
Why Airflow, Posture, and Asymmetry Matter More Than Your Rotator Cuff

Our weight room was in a hallway.
Welcome to the minor leagues!
We had a cable column machine, a rack of dumbbells and some medicine balls lined up along the wall, which was also right next to a batting cage.
This is where our professional baseball players would train.
On this particular day, Markus, our star pitcher from Germany walked into my “weight room” right after he pitched 7 great innings in the game.
“How we doing big man?” I asked.
Without saying a word, he just pointed to a spot on his shoulder.
I knew what this meant.
His shoulder was hurting.
This wasn’t uncommon.
He had just thrown about 100 baseballs as hard as he possibly could and we were four months into the season. There were a lot of miles on that shoulder.
But what was weird to me was how every single pitcher we had was coming in and complaining about pain in the exact same spot.
That was noteworthy to me.
Something we were doing in the weight room…or something that we were NOT doing might be the culprit behind this emerging pattern.
It was my second year in professional baseball at this point, which meant that I had seen nearly 400 baseball games and 95% of my pitchers had pain in the exact same spot.
“What’s going on here?” I thought.
I started to investigate our shoulder strengthening program when I noticed something.
Every baseball pitcher in the world does the same shoulder strengthening exercises.
If you go to any baseball game in America from High School to the Big Leagues, you’ll see guys doing these exercises with a band attached to a fence or with weighted baseballs.
But the minute I peeled back the curtain, I recognized a massive problem with these exercises.
When these baseball players are doing these exercises, they are doing them in a way that the muscle shortens.
Think about a basic bicep curl. Before you start the motion and you are holding the dumbbells by your side, your bicep is long.
But when you begin to do the curl, the bicep is shortening. This is why when you flex your biceps, they look more like a ball.
The major problem here was that when you throw a baseball, the muscles we are targeting (the rotator cuff) are actually lengthening.
This meant we were strengthening these muscles in the complete opposite way that we were supposed to be strengthening them.
I immediately altered their arm strengthening routine and each pitcher that came to me pointing at their shoulder with this familiar pain, had 100% of their discomfort disappear in just a few days.
It was remarkable…and so simple.
My hallway weight room started to develop a reputation as the place where “shoulder pain goes to die.”
In fact, the other Diamondbacks affiliates started to hear rumors about what we were doing and when a new player would be transferred to our roster, they would immediately come in for our special shoulder program.
The Puppetmaster
When I worked for the Diamondbacks, we would always have anatomy quizzes. Our favorite quiz was to see if our strength coaches could name all of the muscles that attach to the shoulder blade.
There are 17 of them.
Here they are…
Biceps
Triceps
Deltoid
Trapezius
Pectoralis Major
Pectoralis Minor
Supraspinatus
Infraspinatus
Subscapularis
Teres Minor
Teres Major
Latissimus Dorsi
Rhomboid
Levator Scapulae
Corocobrachialis
Serratus Anterior
Omohyoid
Let’s look briefly at that last one. The omohyoid. This tiny muscle attaches all the way up under your jaw and somehow makes its way down to the shoulder blade.
But here’s why that’s important.
Imagine you were operating a string puppet. But instead of just a few strings to move, you had 17.
Imagine trying to coordinate all of that movement?
If you pull one string too much, the whole puppet is contorted and thrown off.
It’s tough for you to balance all of those.
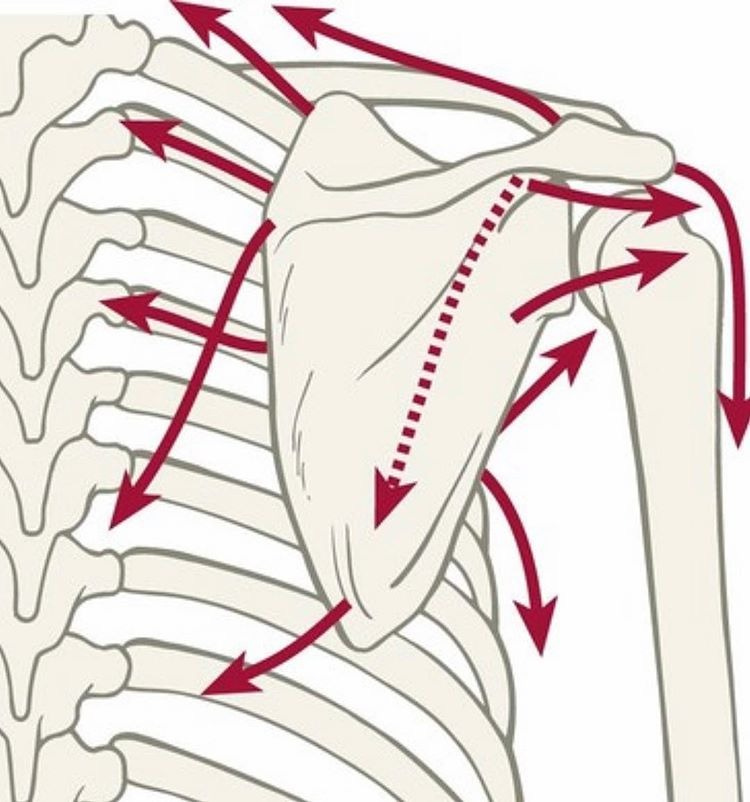
Well, in this case, the shoulder blade (scapula) is the puppet and the muscles are the strings.
If one of these muscles is much stronger than the others, then the whole shoulder blade is going to get messed up.
The shoulder joint is where the humerus bone sits into the glenoid fossa (which is just a convenient indentation in the shoulder blade to hold the humerus bone in place).
If you create imbalances, this joint is going to get contorted and then the labrum will take more stress than it needs, tissue becomes unnecessarily tight and, there is a huge set of nerves called the brachial plexus right up there too that may fire up and cause even more dysfunction.
What Is Actually Happening in Shoulder Pain
Most shoulder pain is not a shoulder problem.
It is a positioning problem.
The shoulder sits on the ribcage. The scapula rests on the ribcage. The humerus articulates with the scapula. If the ribcage is not positioned well, the shoulder never has a stable foundation to move from.
Before we talk about rotator cuffs or impingement, we must talk about the patterns that shape the ribcage itself.
The Pattern Beneath the Shoulder
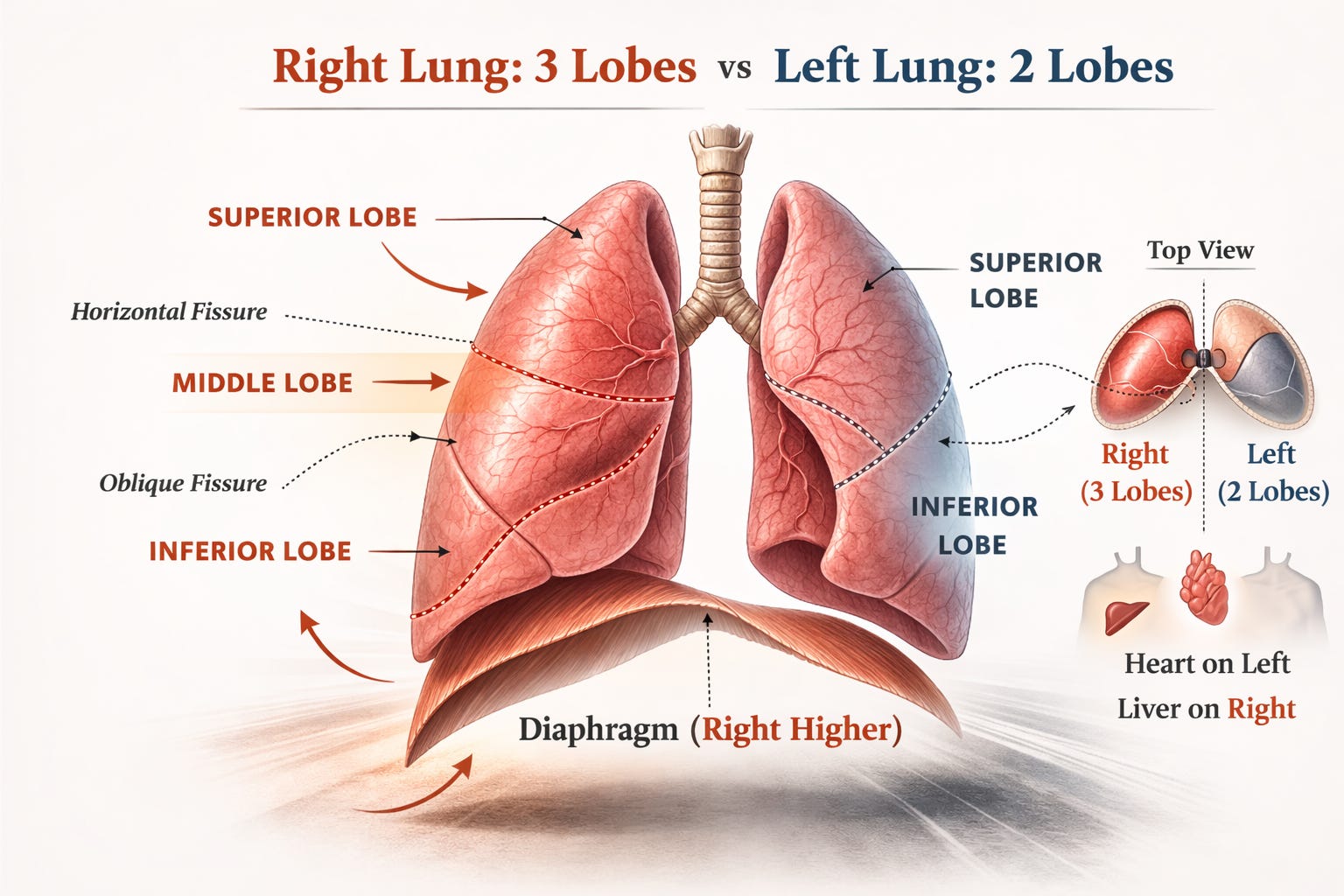
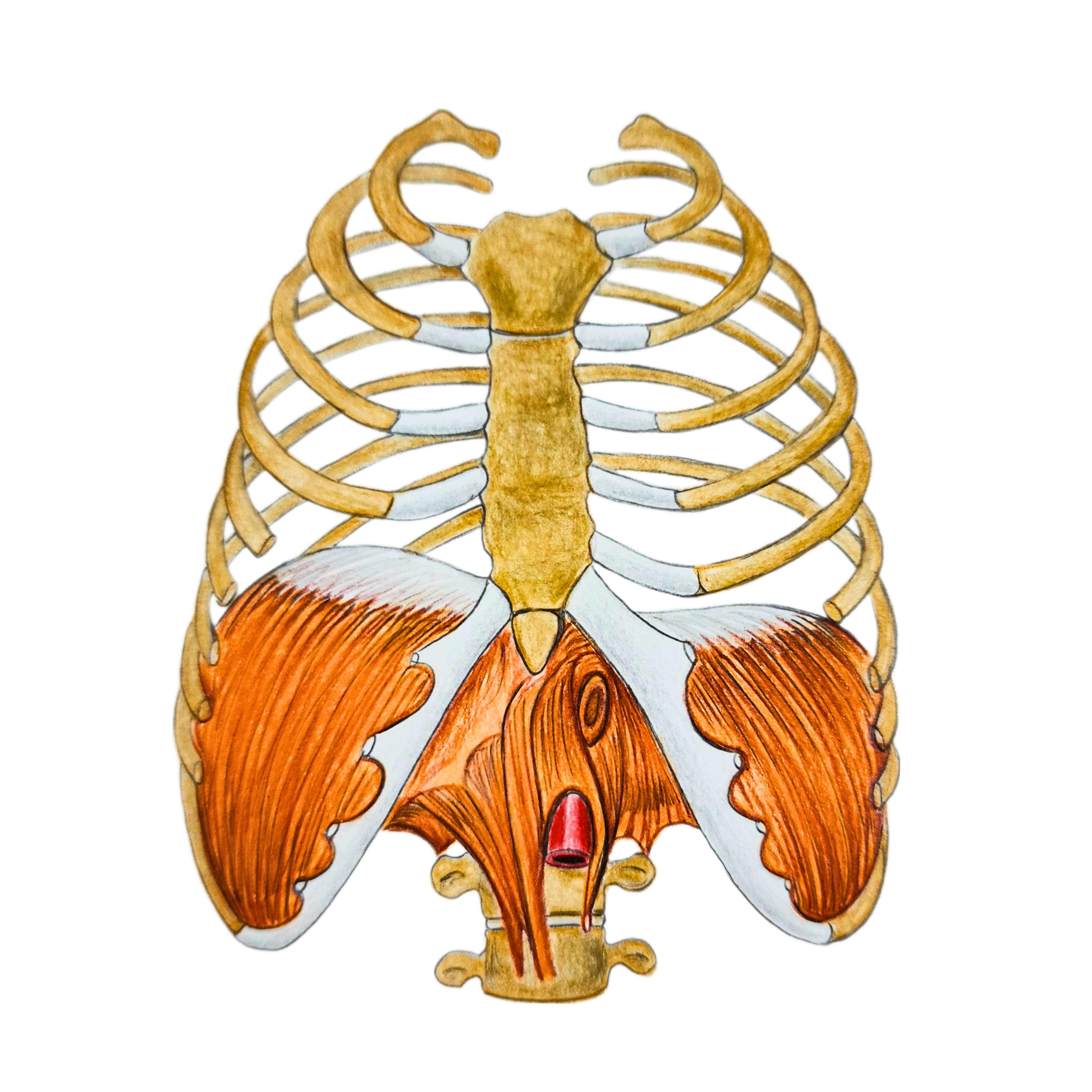
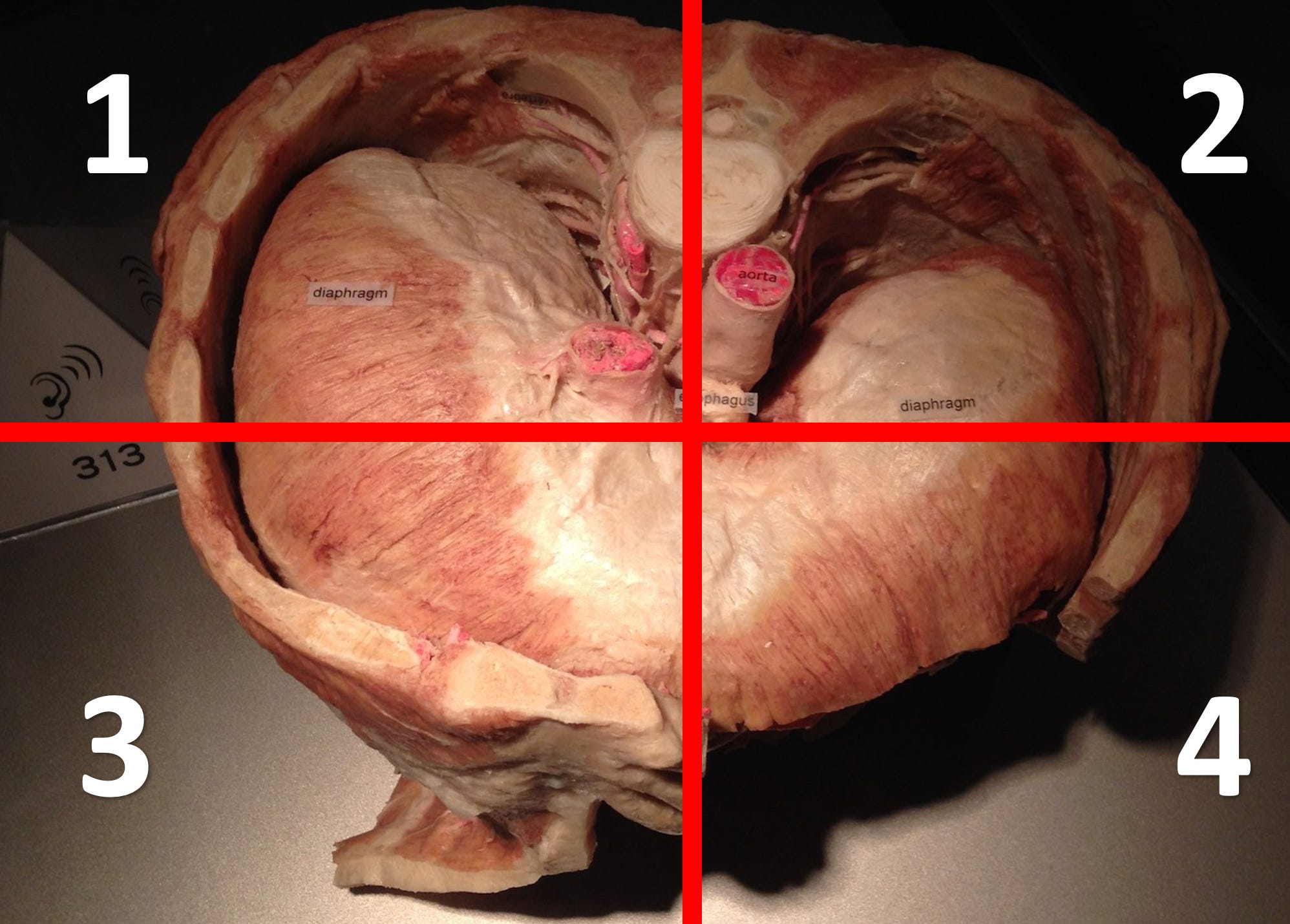
Every human being shares the same anatomical asymmetries. The heart sits on the left. The liver sits on the right. The right diaphragm is larger and stronger than the left. The right lung has three lobes while the left has two.
These asymmetries bias the body into what the Postural Restoration Institute calls the Left AIC and Right BC patterns.
In the Left AIC pattern, the pelvis rotates to the right and becomes very comfortable standing on the right leg. The lumbar spine follows that rotation. Over time, the body struggles to truly shift into left stance.
The upper body must compensate for this rotation. That compensation is the Right BC pattern. The ribcage rotates back to the left in an effort to keep the body facing forward.
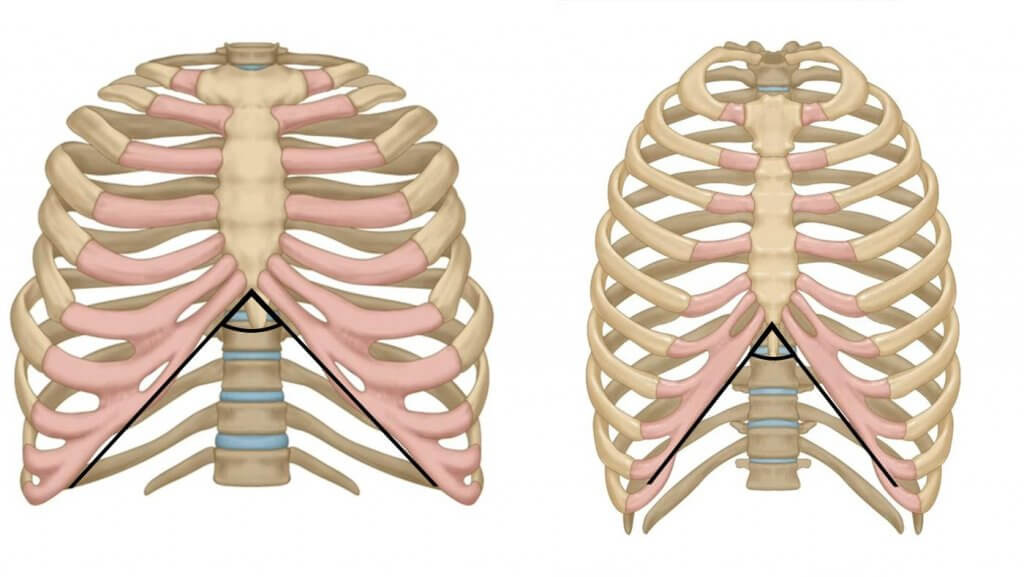
If you look closely at posture in this pattern, you often see a right shoulder that sits lower than the left, a left rib flare in the front, and a right posterior rib hump in the back.

This is not random.
It is predictable.
And the shoulder is sitting directly on top of this asymmetrical platform.
Why the Right Shoulder Is More Vulnerable
The right side of the body has a structural advantage. The right diaphragm is larger. The liver underneath it allows it to sit higher. The right lung has an additional upper lobe that does not exist on the left.
That upper right lobe can be difficult to inflate.
The body prioritizes oxygen above all else. If it senses that the upper right lung is not filling well, it will recruit accessory breathing muscles to create space. The scalenes, sternocleidomastoid, upper trapezius, and subclavius begin pulling on the upper ribs to lift and expand the area.
Over time, those muscles become chronically active.
What feels like shoulder tension is often the neck and upper ribcage trying to breathe.
At this point, treating the shoulder without addressing airflow is incomplete.
Hyperinflation and the Illusion of Good Breathing
Some individuals present differently.
Instead of a single rib flare, they present with a flare on both sides. The infrasternal angle is wide. The lower ribs are expanded. The abdomen rises easily with each breath.
This is a hyperinflated presentation.
These individuals are very good at getting air in, but poor at getting air out. Most of their expansion occurs in the belly and lower ribs because that tissue is easier to move.
The upper ribs, however, remain compressed.
From a shoulder perspective, this is critical.
If expansion never reaches the upper ribcage, the scapula does not have a stable surface to glide on. The shoulder joint becomes unstable. The neck muscles attempt to stabilize what the ribcage cannot.
Clinically, we often see wide infrasternal angles paired with chronic shoulder and neck discomfort.
The issue is not strength.
It is distribution of air.
Asymmetrical Airflow and the Scapula
Breathing should create 360-degree expansion around the entire ribcage.
Because of anatomical asymmetries, that expansion is rarely even.
In the common Right BC presentation, inhalation tends to expand the back right ribcage and the front left ribcage more easily. The back left and front right struggle.
This influences scapular position.
The right scapula often glides forward and becomes more protracted. The left scapula tends to sit further back.
This means what restores one shoulder will not restore the other.
The right shoulder often needs posterior expansion and true retraction mechanics. The left shoulder often needs reaching and protraction to restore balanced airflow.
Cookie cutter shoulder programs fail because they ignore this asymmetry.
Shoulder Pain Is an Airflow Problem
In our experience, shoulder pain is rarely about isolated weakness.
It is about:
A pelvis that cannot alternate stance.
A ribcage that cannot expand symmetrically.
A neck that is working overtime to create space.
A scapula that has lost its stable base.
When airflow is redirected and expansion is restored to both sides of the ribcage, shoulder mechanics improve almost immediately.
The rotator cuff can finally function on a stable platform.
The neck muscles can relax.
The shoulder no longer has to fight for space.
The Solution Is Systemic
Fixing the shoulder requires more than band exercises.
It requires:
Repositioning the pelvis.
Restoring alternating ribcage expansion.
Teaching the upper ribs to fill with air.
Reducing chronic neck tone.
Embedding new patterns through strength and energy production training.
Regulating the nervous system so the body no longer defaults to protective tension.
Like the knee, the shoulder is simply where the alarm bell is ringing.
The real issue is the pattern beneath it.
And once that pattern is addressed, shoulder pain often resolves faster than people expect.
The shoulder is not fragile.
It is simply responding to how you breathe.
Sincerely,
Saint Bartholomew
good old child's pose reach 😉